April 2025 blog
PAs, AAs and the Leng review: many failings of independence...

Bevan model is best
Thatcher wanted compulsory private health insurance
Compulsory expensive premiums paid to an expensive, treatment denying, exclusionary
insurance system is far worse than the efficient universal NHI payments through
the tax system.
A change to social insurance is very costly, ineffective
A & E in one Trust, Medway Maritime Hospital, has
fifty hours corridor waits, and so understaffed that casualties told to shit
in their pants...
A & E needs more cash, more space, receptionists for help and queries, more
chairs and patient couches, more Doctors (not PAs), more nurses, more general
help for toiletting safely...
More treatment cubicles...
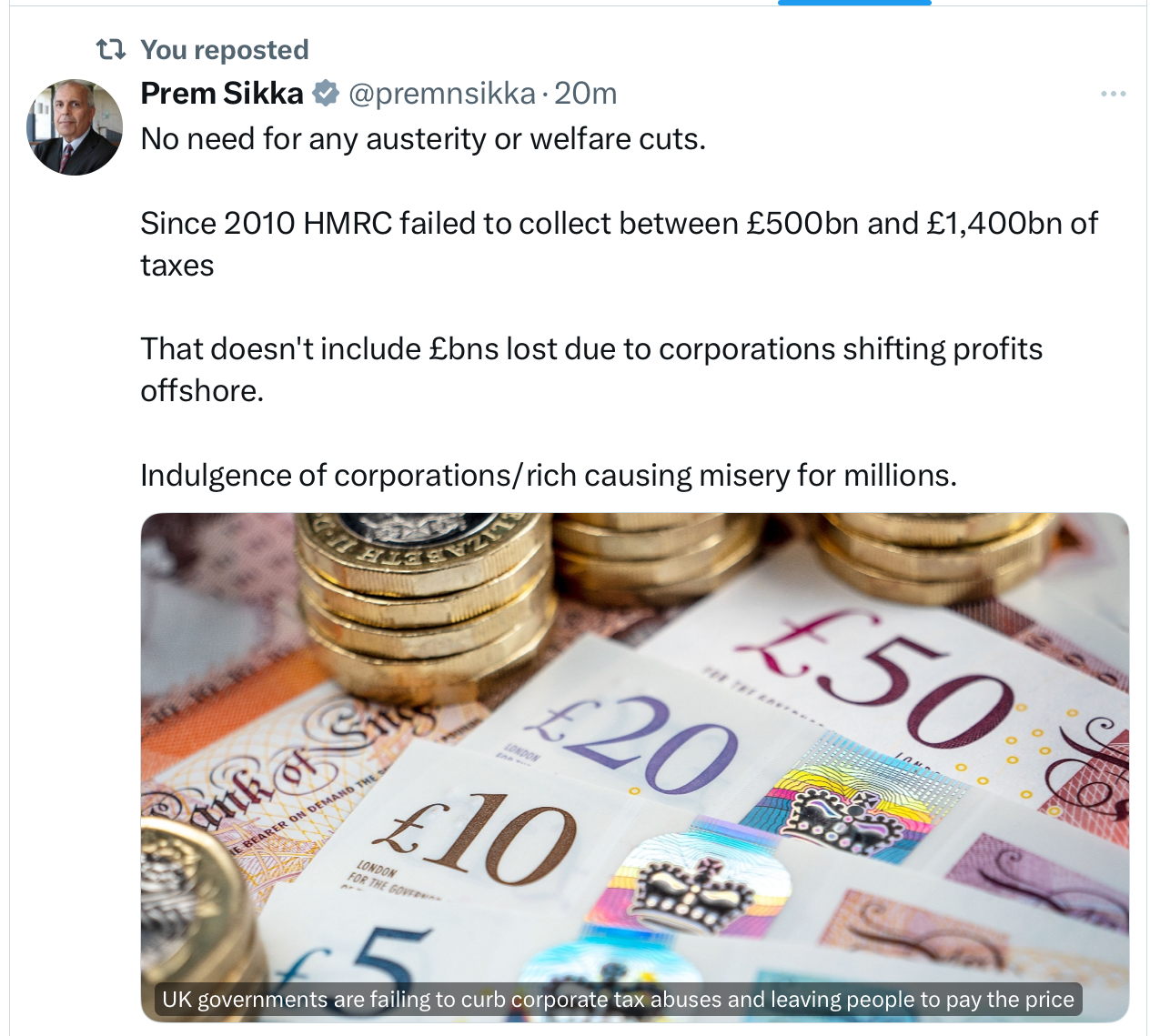
The sane solution is to raise tax-on the wealthy, both
income and assets
to raise income tax, abort the NHI rise on Doctors, Dentists, Care Homes,
Tax oil, stop purchaser provider, tax
Google, Amazon properly
Ban overseas tax havens
Collect all taxes due promptly
Recover Di do's £37 billion inefective
no Test No Trace
Stop wasting money on PAs, AAs-fund GP
practices to hire more GPs
Patient parking clogged up
Parking at most hospitals is ransom by Parking Eye-with
fines going to the company
Buy a 5 acre site, with shuttle bus to the main entrance
Plymouth has a multi storey car park
Free parking for genuine patients
Designated free parking for frontline staff, and subsidised free hot meals and
beveridge 24/7 as MPs have
Pay restoration-as MPs have
On twitter, @EuropeanPowell says Black Rock want the NHS to have an unsustainable debt burden... Starmer and Streeting want privatisation on steroids! BEWARE A SELL OFF OF THE ENTIRE NHS TO BLACK ROCK!!!

Starmer and Streeting cut NHSEngland
Will the overall effect be to depress NHS staff even more, so cuts will be resisted, and staff fight to retain their jobs-while output falls further???
Why-to pretend to Treasury cuts are being made, before demand for more cash
Lansley, 2021 HSCAct: The Health Secretary has no duty to provide a comprehensive Health Service (otherwiser all the profiteers can choose, cherry pick or refuse...)

Mackey-an accountant...
The old privatising Blair privatising hackers-Milburn,
Scrapping NHSEngland
Strategic Health Authorities planned, statistics-very effectively. Many staff were fired,compensated, then rehired...
Jobs cut from NHS restructure rise from 10,000 to between 20,000 and 30,000
42 ICBs thousands of jobs lost
NHSE and DHSC employ 25,000
Jim Mackey: ICBs must reduce by 50%-25,000 people [vaccination BP checks, child
dental health]
to save £400m £750m a year-peanuts
The Lansley reforms
-scrapped RHAs, commissioning by GPs
-created NHSE at arms length from government
-public health from to local government
-creeping privatisation-market based
-handed commissioning to privateers
BMA said “end of the NHS as we know it”
dysfunction of H&SC Act but privateers continued to provide
a lot of talented people at NHSE to lose their jobs
the 220 NHS Trusts ordered to cut corporate services, HR., finance, comms
to prevent overspending by £6.6bn 2025-26
These cuts will remove some services
Why were these people recruited if they are duplicates are unnecessary?
NHSE was formed as the Secretary of State, Health Minister, now has no responsibility to provide a comprehensive NHS (Lansley and 2021 HSCAct), both used to allow profiteers to privatise our NHS.
Unless The Health Secretay has the duty to provide a comprehensive Health Service, and Social Care-theprivateers can refuse to provide some services-like A & E
The whole team in A & E work for the NHS: despite the appalling conditions, every one feels the camaraderie, the unity, trying to provide good care despite the government cuts.
NHSE formed UnAccountable Care DisOrganisations, Clinical Commissioning groups, DisIntegrated Care Boards, which replaced primary care trusts, to provide local clinical services such as GP care
The government allocate rationed cash to the ICBs, who allocate rationed care to patients on GP lists. By demanding ICBs cut budgets-more austerity...
They are like insurance groups
unless this duty is restored-noone in charge
huge number of knowledgeable dedicated staff-fired and rehired
-a distraction, consumes energy, worsens staff morale
-had no understanding of GPs
-from hospitals to community-where no facilities exist-except loading onto GPs
-created CCGs, now ICBs 42 groups to privatise, atomise and ration- now can be abolished
Job losses NHSE 13000
ICBs half fired
Keep Our NHS Public explainer:
NHS England abolished as Starmer and Streeting take ‘control’
14 March 2025 Keep Our NHS Public Cuts, News 3
Credit: Lauren Hurley / No 10 Downing St
Share this post..
Only days after Wes Streeting announced there would be massive cuts in NHS England’s (NHSE) workforce – halved from 13,000 to 6,500 to avoid ‘duplication’ of work by officials at the Department of Health and Social Care (DHSC) – the prime minister Keir Starmer declared on 13 March that NHSE will be entirely abolished.
This was justified on the spurious grounds of a ‘cut to bureaucracy’ and bringing management of the health service ‘back into democratic control’. But what does this mean for the future of the NHS, and is it anything other than more disruptive restructuring (albeit with a populist spin), in the middle of a major NHS crisis?
To answer this question we have to understand what NHSE is, and the context in which this abolition is taking place. While campaigners have often fought for more democracy in NHS decision-making, Starmer and Streeting, the architects of this latest spate of cuts, are enthusiastically in favour of expanding the involvement of the private sector in our NHS.
So who is really taking control of our NHS?
NHSE was set up under the 2012 Health and Social Care Act as an executive non-departmental body (a ‘quango’ organisation that is funded by taxpayers but not controlled directly by central government). It oversaw the budget, planning, delivery and day-to-day operation of the commissioning side of the NHS in England, including compulsory tendering of NHS services in competition between the NHS and the private sector. In other words, it took the money provided by the government and funnelled it into the different parts of the health service – or… private health companies. Although quasi-autonomous, it has been NHSE’s job to translate ministers’ directives into the services people get on the frontline including ensuring that NHS key waiting times, such as the targets for maximum four-hour wait for A&E care and 18-week wait for hospital treatment, were delivered.
In practice, the Secretary of State for Health and Social Care is now taking back the duty to provide comprehensive health services, abolished by the 2012 Lansley Act. Campaigners have demanded the return of this accountability to Parliament and the electorate ever since 2012, but Streeting’s new powers do not give cause for celebration.
Starmer used abolition of NHSE as the main example of how he will remedy the ‘overstretched’ and ‘unfocused’ state. This comes amid major cuts to disability benefits and job cuts to the civil service.
The parallels with events unfolding in the US are chilling. Some Labour aides
have taken to referring to the agenda as “project chainsaw“, a reference
to the dramatic and legally questionable cuts to the US executive branch currently
being overseen by Elon Musk.
Elon Musk wields a chainsaw, February 20 2025
We have in the past challenged the relevance and usefulness of NHSE as a quango, viewing it as a vehicle for fragmenting the NHS and opening it to privatisation; we should not therefore mourn its demise. It is now starkly evident that the NHS buck stops with Streeting. Huge numbers of staff are facing redundancy and the Government has behaved disgracefully in the timing of announcements. The loss of so many experienced staff may save some money short-term – a tiny fraction of what the NHS needs to be rebuilt – but it will have a negative impact on how the NHS is run nationally. The 42 local Integrated Care Boards are stripped bare, instructed merely to fulfil the function of commissioning NHS services, and under direction to increasingly consider outsourcing to the private sector.
The central question remains – how is Labour going to fix the NHS as it promised and as the electorate demands?
Clearly appropriate concern over not meeting targets for NHS performance has fuelled the desire for more centralised control while overemphasising modest gains. In March, we saw that the 2 million more appointments in the first seven months of office were trumpeted as Labour delivering on its manifesto promises. This will have made but a small dent in the waiting list of 6.25 million people waiting for 7.43 million treatments and a lot more will have to be done to shift the dial. Meanwhile, other manifesto commitments including building new hospitals and rolling back outsourcing have simply been abandoned.
Those now taking charge in the DHSC include Alan Milburn, Paul Corrigan and
others from the Blair-Brown years. They are strongly associated with the policies
of privatisation and marketisation of health care which substantially failed
in the 2000s. Then, it was the serious investment in the NHS itself that ended
long waiting lists and restored public satisfaction. Instead of learning from
Labour’s past experience in office, we are seeing an emphasis on a return
of private investment to solve lack of capital funding and billions invested
to expand the private sector with incentives for providers. Even if there might
be some scope for efficiency savings from fewer workers duplicating roles, going
back to failed policies coupled with even more drastic constraints on revenue
funding is unlikely to deliver meaningful change.
Wes Streeting, in conversation with Andrew Marr, for Policy Exchange fringe
event
It is difficult at present to see the abolition of NHSE and thousands of redundancies as anything other than a move to facilitate Labour plans for ’reform’. The bad news is that ‘reform’ looks like another reorganisation where the beneficiaries will be private companies as an increasingly fragmented NHS is opened up to commercial interests. It’s no surprise that NHSE staff are ‘in shock and awe’ at the scale of the job cuts, which have spiralled from 2,000 just weeks earlier to 6,500 last week to now, with 10,000 job losses said to make £500 million savings.
Now in our 20th anniversary year, KONP is needed more than ever to put the case for a well-resourced publicly funded, provided and accountable NHS based on its founding principles. After this power grab, it is clearer than ever that Streeting, as Secretary of State, and the Labour Government will be the ones held to account if after all their commitment to ‘change’ they fail to restore a healthy NHS to meet the needs of the population.
In case you missed it: KONP co-chair Tony O’Sullivan on Novara Media
responding to NHSE news here
JOIN THE PROTEST: Tuesday 25 March 6:30pm outside Conway Hall, 5 Red Lion St,
London WC1R 4RL
Keep Our NHS Public, Just Treatment, Socialist Health Association and NHS Workers
Say NO, have called a protest outside Conway Hall on March 25, from 6:30pm where
Wes Streeting and Guardian Political Editor, Pippa Crerar, are holding a discussion
called ‘England’s health and social care system is in crisis. How
does Labour plan to turn it around?’
Streeting must listen to the demands of NHS campaigners, patients, and workers, commit to ending the private involvement that ultimately weakens our NHS and invest urgently to rebuild the NHS.
Please join us outside Conway Hall on 25 March from 6:30pm 8:30 to let Wes Streeting know the NHS is here to stay, privatisation no way!
Julia Patterson, EveryDoctor
There is endless reporting about NHS England at the moment, because Keir Starmer has just announced that it will be abolished. But somehow, in all of these conversations about the NHS, the NHS itself has been lost. Somehow, in critiquing the quango, we’ve lost sight of why the quango has swelled to such a size. And somehow, by pointing their fingers at NHS England, politicians have managed to remove themselves from the firing line…
QUICK NOTE FOR MY LOVELY READERS! Lots of my readers have asked me to add a “donate” button to my newsletters, so that they can add a tip when they find a newsletter particularly interesting or informative. This is so kind - so there’s a button at the bottom to donate if you would like to. All donations support the research and writing that goes into this newsletter! Ju
Abolishing NHS England may leave Streeting with nowhere to hide...
Since Keir Starmer’s announcement this Thursday that NHS England would be abolished, there has been an awful lot of discussion. Everyone, it seems, has had something to say about it. We’ve had endless articles, think pieces and statements from everyone I can think of in the worlds of politics, media, campaigning and health. I sat in bed this morning to go through my Google alerts, and read dozens of pieces on the topic.
Much of the coverage has been deeply political. Comparisons are being made between Labour and the Tories. Robert Jenrick’s opinion on all of this is somehow making the news. Much of the focus being sucked up by broader conversations; general talk about quangos, or talk of ‘inefficiency’, or the age-old complaint that the NHS has too many managers, and that it’s necessary to cut things back to create a ‘leaner’ health service.
It is in this mix of commentary that several camps seem to have emerged; camps trying to explain their take on what’s going on, and predicting what will come next. There’s the ‘pro-Streeting’ camp - celebrating his bold decisions and even claiming that this move could end NHS privatisation. There’s a Streeting-skeptic group (a camp into which I fall), who feel it is highly unlikely that less privatisation is on the cards with these new changes, and feel worried about politicians enacting a power grab of the NHS. And there’s a third group, a much quieter group, who have important things to say who aren’t making the headlines at all.
Somehow, in all of these conversations about the NHS, the NHS itself has been lost. Somehow, in critiquing the ‘quango’, we’ve lost sight of why the quango has swelled to such a size. And somehow, by pointing their fingers at NHS England, politicians have managed to remove themselves from the firing line…
It’s true that NHS England is absolutely enormous. The Independent has written a really interesting article about quangos (available here), which contains this quote: “The latest data on the UK’s quangos comes from 2023, when there were 304 arms-length bodies in operation. Of these, the ten largest received the vast majority of funding - 92 per cent … NHS England was by far the largest of these, receiving £159.26 billion in 2023. The next largest, the Education and Skills Funding Agency, received £67.46 billion.”
So it’s massive, and it’s sprawling, and it costs the taxpayer a huge amount of money. It also employs an enormous number of people (estimates in the newspapers set this at around 13,000 employees in total). However, there’s been very little in those same newspapers about the roles those employees actually perform. I mentioned some of the work NHS England does here on Substack on Thursday, but the remit is extensive; here are some other examples in their own words - they:
“…allocate the £134 billion of funding agreed by government
and Parliament to local NHS systems to enable the NHS to deliver high quality
care and get best value for the taxpayer”
“…run the world-leading NHS Genomic Medicine Service, which in 2023/24
delivered 810,000 genomic tests for over 7,000 rare diseases, and over 200 cancer
clinical indications”
“…run the NHS App, which has been downloaded by over 36 million
people, with an average of 10 million people logging into it each month to manage
their health needs; that is in addition to running NHS 111 online and NHS.UK
– trusted digital services that allow patients to conveniently access
care”
Could these projects be run by another body, such as the government’s Department of Health and Social Care (DHSC)? Absolutely, of course that’s possible. But will transferring this work to the DHSC also generate its own bureaucracy and enormous costs? Yes, that will absolutely happen.
This government, after all, speaks in big terms about cutting back waste, reform, and only investing in what’s needed. But are they going to eliminate the country’s vaccination programme? Our ability to recruit patients into clinical trials? Our NHS Genomics Medicine Service (“which in 2023/24 delivered 810,000 genomic tests for over 7,000 rare diseases, and over 200 cancer clinical indications”)? I sincerely hope not. So someone’s going to have to do that work. Unless Streeting is going to eliminate these programmes too, he is simply moving pieces around a chessboard.
There’s been a lot of talk in the newspapers about his plan to eliminate jobs which have been duplicated, because there are similar teams in the Department of Health and Social Care and NHS England, and perhaps that’s the case. But the situation is definitely being exaggerated, because the most common example I’m seeing referenced is that both organisations have a communications team. Of course both organisations have a communications team, because they are running different projects and are communicating about different things.
We can’t talk about this situation without talking about how it’s been handled by Streeting and Starmer; because it’s been handled really badly. First we were told that the NHS leadership was stepping down and that there would be some job cuts. Then we were told that NHS England would be abolished, and now it’s emerged that the changes extend far beyond NHS England itself. The Guardian have been covering this situation closely, and one of their pieces contains this quote:
“The jobs cull from the government’s radical restructuring of the
NHS will be at least twice as big as previously thought, with other parts of
the health service now being downsized too … The staff shakeout caused
by NHS England’s abolition and unprecedented cost-cutting elsewhere will
mean the number of lost posts will soar from the 10,000 expected to between
20,000 and 30,000.”
…while another explains what is happening in the 42 integrated care boards around the country:
“Sir Jim Mackey, NHS England’s incoming new chief executive, has
told the ICBs to cut their running costs by 50% by the end of the year. ‘Given
ICBs employ 25,000 people, that means that half of them are going to go,’
a senior NHS official said. That could lead to 12,500 posts being lost.
In addition, Mackey has also ordered the 220 NHS trusts that provide care across England to cut the number of people working in corporate services, such as HR, finance and communications. That could lead to thousands more officials losing their jobs, insiders say.
Senior figures running ICBs say the order to halve their running costs will make it impossible for them to undertake the full range of their activities, which include funding vaccination programmes, offering blood pressure checks and improving children’s dental health. ICBs have recently finished reducing their budgets by 20% as part of a previous round of cost-saving.”
I was hearing from staff working at both NHS England and various Integrated Care Boards on Friday, all of whom spoke of the confusion and upset locally as they were called into urgent meetings and told that huge job cuts would be made, without being told specifically who was going to go and when. What needs to be emphasised is how poorly planned this has been, and how its execution alone it will have a negative impact on the NHS itself. What gets lost in these high-level conversations about efficiencies and slash-and-burn politics is the human element of all of this. The NHS and its associated bodies are actually a group of people who are engaged in work towards a collective goal. If you start hacking away at that without clear, strong, humane leadership, you will damage morale, damage loyalty, and damage the very productivity which you claim to be working to advance.
Ultimately, despite their political grandstanding, and Keir Starmer’s big talk of overhauling Britain’s “flabby state”, it will be impossible to reduce the quangos while the public services themselves remain sprawling and fragmented. It is politicians, not quangos, who have broken the NHS into the many small parts which struggle to communicate properly with one another. It is politicians, not managers, who have outsourced thousands of services to external providers, including major private corporations, which has embedded layers upon layers of bureaucracy on NHS managers and procurement teams. It is politicians, not NHS staff, who have put the NHS through endless reforms spawning the complex structures that now run the NHS. Unless they confront this, they won’t be able to streamline the NHS in the way they want.
I’m concerned that by eliminating NHS England it will be even easier for ministers to make decisions for the NHS which make them look good in the short-term, while ignoring the difficult conversations to make the NHS sustainable in the long-term. I’m concerned that it will make it even easier for them to ignore public health projects for example, and fail to build NHS hospitals and invest in the GP surgeries that the public sorely needs.
But I’m also curious about whether Wes Streeting has really considered
the added scrutiny he will have to endure when NHS England is gone. In recent
years, NHS England has provided a very effective buffer for politicians - they
can decide on budgets and policy commitments and pass them onto NHS England,
who are ultimately responsible for delivering them safely. Should waiting lists
continue to increase, and the winter crises continue to recur year on year,
then finally it will be the politicians who will have to face the music. They
will no longer have a convenient organisation to blame, and will have to confront
the fact that it was politicians’ decisions that have been costly, flabby
and inefficient all along.
High Intensity: Private teams? Julia Patterson Every Doctor
https://jujuliagrace.substack.com/p/is-nhs-privatisation-about-to-accelerate-87a?utm_campaign=email-post&r=2hqe8s&utm_source=substack&utm_medium=email
Welfare spending
Immigrant NHS workers keep our NHS and Social care functioning
but it is wrong to import skilled workers from countries who need them more
urgently
Immigration control-by having immigration visa centres in France, and agreement
from France to accept returns the same day is sensible.
Work and Pensions Secretary
-school leavers into benefits
-sickfluencers to take full advantage
-£5 million just a drop in the ocean Welfare & pensions £300
billion, 10% of GDP
-Abolish Work Capability Assessment
-score fit or unfit to work
-any work found-lose benefits
All cases now by Personal Independence Payment benefits for disabled and unable
to work
-right to try
-Overhaul Universal Credit
-Limited Capability for Work cut from £97 to £50 from April 2026
-if qualified before April 2026-receive old figure
Gen z 1 in 8 out of work
60,000 18-22 receive LCWRA
hundreds of thousands receive PIP
25-34 disabled risen doubled decade from 11% to 20%
also older people 26% to 30% 50-64
raising eligibility 18-22
pip 16-18
legally contentious
Stricter PIP assessment
3 million get PIP £21.8 billion
4.2 million to 34 billion a year
£500 million for ADHD
Assessment by a Doctor-from a different practice, face to face, not contractors,
not by video or phone
Sickfluencers
Access to Work £69,000 initially by blind deaf, but sickfluencers ADHD,
support workers hundreds an hour
£258 million
£712 million end of decade
37,000 23-24 to 84,000 by 29-30
average award £6,600 to £8,500
taking money from carers and support workers
wealth tax before cutting benefits
The domino effect: PIP cuts reduce lots of other benefits...
Losing PIP lose free prescriptions, council tax deductions, unpaid carer loses carer's allowance
savaging two main strands of support...
Is this small saving worth the candle?

The brilliant Lowdown website has articles by John Prentis
The Lowdown lowdownnhs.info
Sub co's subcontracting loyal NHS staff to private companies-worse terms, conditions and protection...